


1Department of Dermatology, Hokkaido University Graduate School of Medicine, N15 W7, Kita-ku, Sapporo 060-8638, 2Department of Surgical Pathology, Hokkaido University Hospital, 3Sapporo Dermatopathology Institute, 4Department of Surgical Pathology, Sapporo Medical University School of Medicine, and 5Hamaoka Dermatology Clinic, Sapporo, Japan. *E-mail: yfujita@med.hokudai.ac.jp
A 16-year-old Japanese boy presented to our hospital with a subcutaneous nodule on the right palm that had developed over 4 months. He reported a history of “ganglion cyst” in the same area that had been treated with drainage at another clinic 3 years earlier.
Clinical examination revealed a tender, mobile subcutaneous nodule 12×12 mm on the right palm near the antithenar eminence. Slight, poorly demarcated pigmentation was observed on the surface of the nodule (Fig. 1).
Fig. 1. Clinical presentation. A tender, mobile subcutaneous nodule on the right palm (arrow).
Ultrasonography confirmed that there was no blood flow inside the tumour. Surgical excision was performed under the clinical diagnosis of recurrent ganglion cyst. The excised specimen revealed the proliferation of atypical cells with vesicular nuclei and mild myxoid areas (Fig. 2A), mixed with prominent inflammatory cell infiltrates of lymphocytes and plasma cells (Fig. 2B). Large cells with atypia were also noted, part of which resembled Reed–Sternberg cells (Fig. 2C). Immunohistochemically, these atypical cells were positive for CD68 (KP-1, PGM-1) and negative for alpha-smooth muscle actin, CD34 and AE1/AE3.
Fig. 2. Histopathology of the excised nodule. (A) Fibrous areas with mucin deposition surrounded by inflammatory cells (haematoxylin and eosin staining, original magnification ×100). (B) Inflammatory cells composed of lymphocytes, plasma cells and eosinophils (original magnification ×200). (C) Large cells with atypia (arrows) are noted, with Reed–Sternberg-like cells (arrowhead) (original magnification ×400).
What is your diagnosis? See next page for answer.
Diagnosis: Myxoinflammatory fibroblastic sarcoma
Myxoinflammatory fibroblastic sarcoma (MIFS) is a rare, low-grade, soft-tissue sarcoma that was first described by several different groups in 1998 (1–3). Fewer than 200 cases have been reported (4). MIFS is clinically characterized by its appearance on distal extremities. Tejwani et al. (5) reported that there is no predilection for sex or age, with ages ranging from 4 to 87 years. Histologically, MIFS is composed of hypocellular areas and dense cellular areas. The former areas are myxoid and fibrous. The latter areas comprise prominent inflammatory cell infiltrates, such as eosinophils, neutrophils, lymphocytes and plasma cells, as well as large atypical tumour cells, including Reed-Sternberg-like cells and lipoblast-like cells (1, 4, 6). These histological characteristics were consistent with the present case.
Immunohistochemically, no specific findings have been reported. The tumour cells are positive for vimentin, focally positive for CD34 and CD68, and negative for S-100 protein, alpha-smooth muscle actin, muscle-specific actin, AE1/AE3, CAM 5.2, desmin, CD15, CD45, HMB45, Epstein-Barr virus latent-membrane protein, EMA and GFAP (1–4, 7).
Because of its clinical presentation and histological characteristics, even experienced dermatologists and pathologists can misdiagnose MIFS as ganglion cyst, tenosynovitis and non-neoplastic disease (5). The present case was initially diagnosed as “ruptured ganglion cyst.”
MIFS has been reported to have a relatively low potential for metastasis, but a high risk of recurrence. The metastasis and recurrence rates have been reported as 3.1% and 31.3%, respectively (5). Lombardi et al. (8) reported that cancer-related death was seen in only one case of 138 patients with MIFS. No standard treatment protocol exists. Ieremia et al. (4) recommend wide local excision with 5-year follow-up observation for MIFS. Some reports have indicated that surgical excision with radiation therapy maintained a good clinical course (5, 9).
Although MIFS is rare, it is important for clinical dermatologists to keep it in mind when repeated recurrences of “ganglion cyst” are observed, especially on the distal extremities. Excision and skin biopsies will help diagnose MIFS correctly with characteristic histopathological findings.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize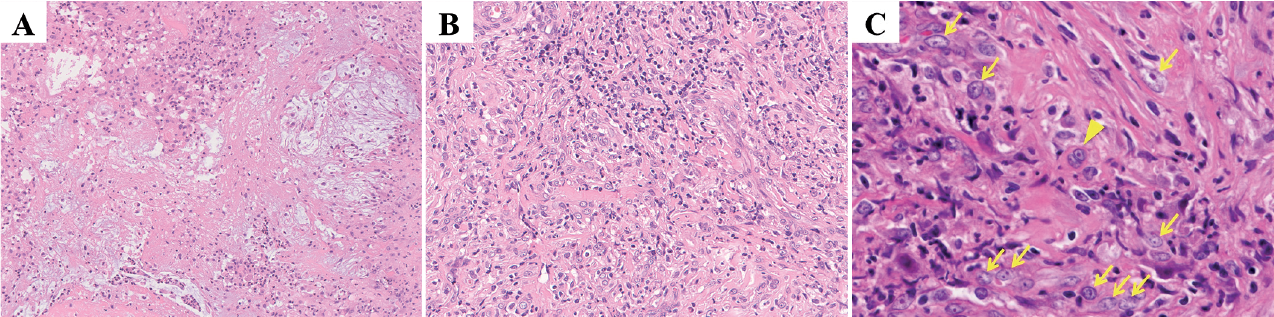 Click to show fullsize
Click to show fullsize